Key element of CPR missing from guidelines
July 28, 2014
Share
By Anne Craig, Communications Officer
Removing the head tilt/chin lift component of rescue breaths from the latest cardiopulmonary resuscitation (CPR) guidelines could be a mistake, according to Queen’s University professor Anthony Ho.
Traditional CPR guidelines for out-of-hospital cardiac arrest by lay bystanders include rescue breaths. These are delivered using a combination of head tilt/chin lift and mouth-to-mouth breathing. Under the new guidelines, these are now omitted.
 Anthony Ho says CPR guidelines are missing a key component.
Anthony Ho says CPR guidelines are missing a key component.“Wholesale elimination of ventilation from CPR by laypersons for adults with out-of-hospital cardiac arrest may be misguided,” says Dr. Ho (Anesthesiology and Perioperative Medicine), who is also at Kingston General Hospital.
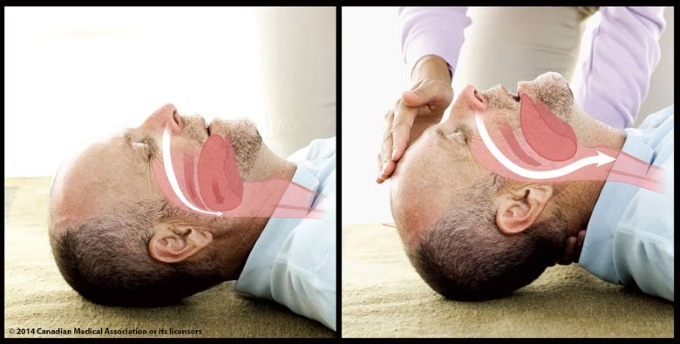
“It is important to remember that rescue breathing is a two-part intervention: head-tilt-chin-lift and delivery of rescue breaths. Head-tilt-chin-lift, the key to overcoming obstruction in the upper airway in unconscious patients, is not the reason for all the undesirable effects of rescue mouth-to-mouth breathing.”
The new guidelines, issued by the International Liaison Committee on Resuscitation in 2010, recommend CPR using only chest compressions if performed by untrained bystanders. Mouth-to-mouth resuscitation was removed from the guidelines as it can delay or interrupt chest compressions, too much ventilation could be provided, and bystanders may be reluctant to perform it.
With a survival rate of only 14 per cent for compression-only CPR, Dr. Ho says there is a lot of room for improvement. Dr. Ho’s commentary was published in the most recent edition of the Canadian Medical Association Journal.